Overview
This Guidelines summary covers key recommendations related to the use of emergency contraception (EC). Included are two useful decision-making algorithms, as well as recommendations on when EC is indicated; the responsibilities of EC providers; the relative effectiveness of different EC methods; relevant drug interactions; contraindications for EC use; specific considerations for women who breastfeed; EC use more than once in a cycle; advice regarding future contraception.
This summary only covers key recommendations for primary care. For a complete set of recommendations, refer to the full guideline.
Reflecting on Your Learnings
Reflection is important for continuous learning and development, and a critical part of the revalidation process for UK healthcare professionals. Click here to access the Guidelines Reflection Record.
When Is EC Indicated?
- Women who do not wish to conceive should be offered EC after unprotected sexual intercourse (UPSI) that has taken place on any day of a natural menstrual cycle
- Women who do not wish to conceive should be offered EC after:
- UPSI from day 21 after childbirth (unless the criteria for lactational amenorrhoea are met)
- UPSI from day 5 after abortion, miscarriage, ectopic pregnancy, or uterine evacuation for gestational trophoblastic disease
- Women who do not wish to conceive should be offered EC after UPSI if their regular contraception has been compromised or has been used incorrectly.
Provision of Emergency Contraception
What Are the Responsibilities of EC Providers?
- EC providers who cannot offer all EC methods should give women information regarding the other methods and signpost them to services that can provide them. If a woman is referred on for a copper intrauterine device (Cu-IUD), oral EC should be given at the time of referral in case the Cu-IUD cannot be inserted or the woman changes her mind
- Providers of oral EC should advise women that oral EC methods do not provide contraceptive cover for subsequent UPSI and that they will need to use contraception or abstain from sex to avoid further risk of pregnancy
- Women requesting EC should be given information regarding all methods of ongoing contraception and how to access these.
How Effective Are the Different Methods of EC?
- EC providers should advise women that the Cu-IUD is the most effective method of EC
- EC providers should advise women that ulipristal acetate EC (UPA-EC) has been demonstrated to be effective for EC up to 120 hours after UPSI
- EC providers should advise women that levonorgestrel EC (LNG-EC) is licensed for EC up to 72 hours after UPSI. The evidence suggests that LNG-EC is ineffective if taken more than 96 hours after UPSI
- EC providers should advise women that UPA-EC has been demonstrated to be more effective than LNG-EC
- EC providers should advise women that the available evidence suggests that oral EC administered after ovulation is ineffective.
What Is the Effect of Weight/BMI on the Effectiveness of EC?
- Women should be informed that the effectiveness of the Cu-IUD is not known to be affected by weight or body mass index (BMI)
- Women should be informed that it is possible that higher weight or BMI could reduce the effectiveness of oral EC, particularly LNG-EC.
What Drug Interactions Are Relevant to Use of EC?
- EC providers should advise women using enzyme-inducing drugs that the effectiveness of UPA-EC and LNG-EC could be reduced
- Women requiring EC who are using enzyme‑inducing drugs should be offered a Cu-IUD if appropriate. A 3 mg dose of LNG can be considered but women should be informed that the effectiveness of this regimen is unknown. A double dose of UPA‑EC is not recommended
- EC providers should be aware that the effectiveness of UPA-EC could be reduced if a woman takes progestogen in the 5 days after taking UPA-EC
- EC providers should be aware that the effectiveness of UPA-EC could theoretically be reduced if a woman has taken progestogen in the 7 days prior to taking UPA-EC.
Are There Any Contraindications/Restrictions to Use of EC?
- EC providers should be aware that the contraindications to insertion of a Cu-IUD for EC are the same as those for routine IUD insertion
- EC providers should be aware that UPA‑EC is not suitable for use by women who have severe asthma controlled by oral glucocorticoids.
Are There Any Specific Considerations for Women Who Are Breastfeeding and Require EC?
- EC providers should be aware that breastfeeding women have a higher relative risk of uterine perforation during insertion of intrauterine contraception than non‑breastfeeding women. However, the absolute risk of perforation is low
- Breastfeeding women should be advised not to breastfeed and to express and discard milk for a week after they have taken UPA-EC
- Women who breastfeed should be informed that available limited evidence indicates that LNG-EC has no adverse effects on breastfeeding or on their infants.
What Methods of EC Should Be Offered to a Woman Who Has Had UPSI and Wishes to Avoid Pregnancy?
- See decision-making algorithms below to facilitate choice of EC
- All women requiring EC should be offered a Cu-IUD if appropriate as it is the most effective method of EC
- EC providers should be aware that a Cu-IUD can be inserted up to 5 days after the first UPSI in a natural menstrual cycle, or up to 5 days after the earliest likely date of ovulation (whichever is later)
- If a Cu-IUD is not appropriate or not acceptable, women should be advised that oral EC should be taken as soon as possible if there has been UPSI within the last 5 days
- EC providers should consider UPA-EC as the first-line oral EC for a woman who has had UPSI 96–120 hours ago (even if she has also had UPSI within the last 96 hours)
- EC providers should consider UPA-EC as the first-line oral EC for a woman who has had UPSI within the last 5 days if the UPSI is likely to have taken place during the 5 days prior to the estimated day of ovulation
- EC providers should advise women that the available evidence suggests that oral EC administered after ovulation is ineffective
- Adolescents who need EC should be offered all methods of EC including the Cu-IUD
- Women requiring EC after sexual assault should be offered all methods of EC including the Cu-IUD.
Can Oral EC Be Used If There Has Also Been UPSI Earlier in the Cycle?
- EC providers can offer a woman UPA‑EC or LNG‑EC if she has had UPSI earlier in the same cycle as well as within the last 5 days, as evidence suggests that UPA‑EC and LNG‑EC do not disrupt an existing pregnancy and are not associated with fetal abnormality.
Can Oral EC Be Used More Than Once in a Cycle?
- If a woman has already taken UPA-EC once or more in a cycle, EC providers can offer her UPA-EC again after further UPSI in the same cycle
- If a woman has already taken LNG-EC once or more in a cycle, EC providers can offer her LNG-EC again after further UPSI in the same cycle
- EC providers should be aware that if a woman has already taken UPA-EC, LNG-EC should not be taken in the following 5 days
- EC providers should be aware that if a woman has already taken LNG-EC, UPA-EC could theoretically be less effective if taken in the following 7 days.
What Should Women Be Advised Regarding Future Contraception?
- EC providers should advise women that the Cu-IUD provides effective ongoing contraception
- EC providers should advise women that oral EC methods do not provide ongoing contraception
- EC providers should advise women that after oral EC there is a pregnancy risk if there is further UPSI and ovulation occurs later in the same cycle
- After taking LNG-EC, women should be advised to start suitable hormonal contraception immediately. Women should be made aware that they must use condoms reliably or abstain from sex until contraception becomes effective
- Women should be advised to wait 5 days after taking UPA-EC before starting suitable hormonal contraception. Women should be made aware that they must use condoms reliably or abstain from sex during the 5 days waiting and then until their contraceptive method is effective
- If a woman and her EC provider estimate that UPSI is unlikely to have occurred during her fertile period, she may consider the option of using LNG-EC with immediate start of hormonal contraception rather than UPA-EC with delayed start of hormonal contraception.
Decision-Making Algorithms
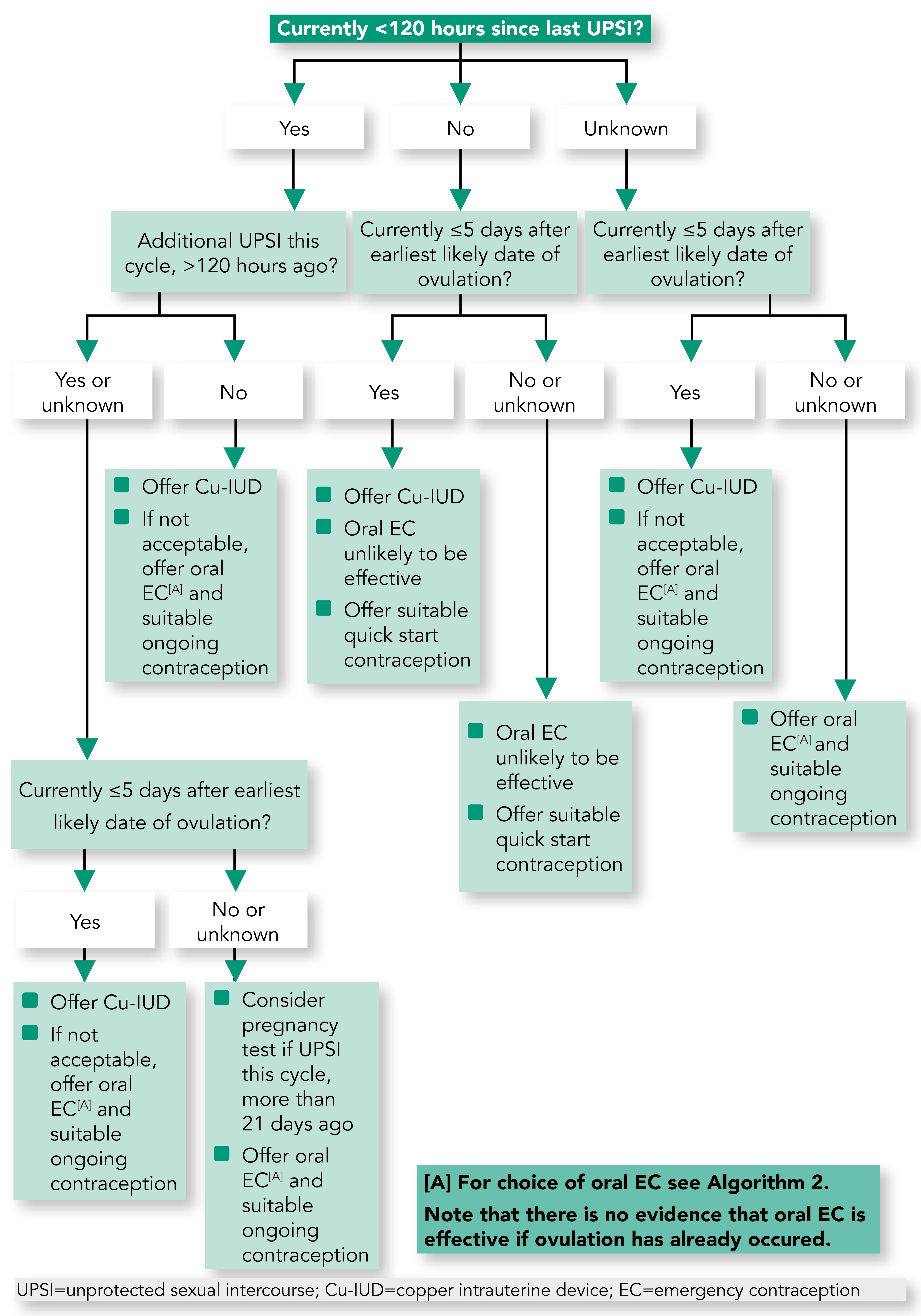
Algorithm 1: Decision-Making Algorithm for EC: Copper Intrauterine Device Versus Oral EC
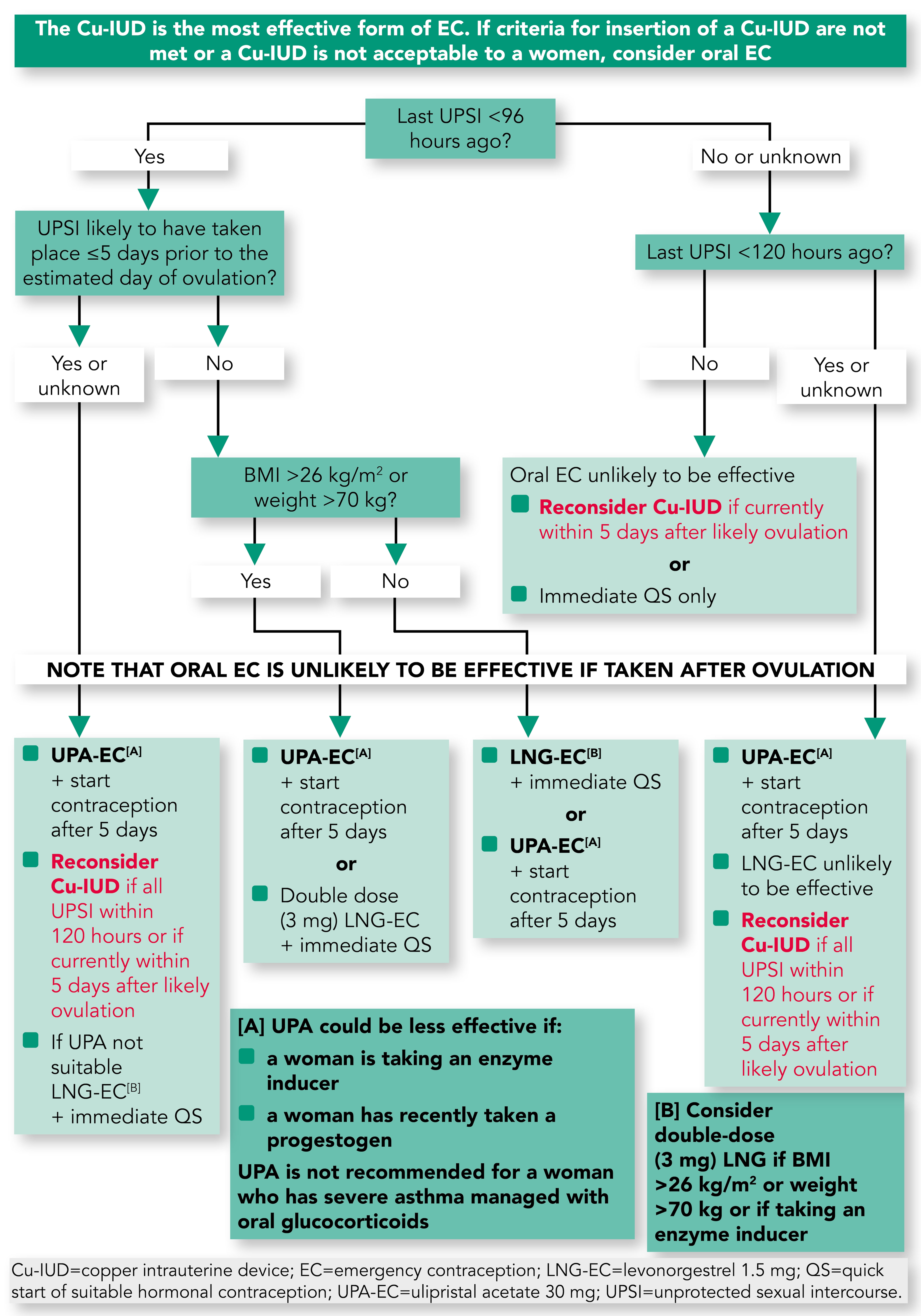
Algorithm 2: Decision-Making Algorithm for Oral EC: Levonorgestrel EC Versus Ulipristal Acetate EC