

This guideline sets out an antimicrobial prescribing strategy for adults, young people, and children aged 72 hours and over with impetigo. It aims to optimise antibiotic use and reduce antibiotic resistance.
For further information, view the full guideline.
Impetigo—Antimicrobial Prescribing
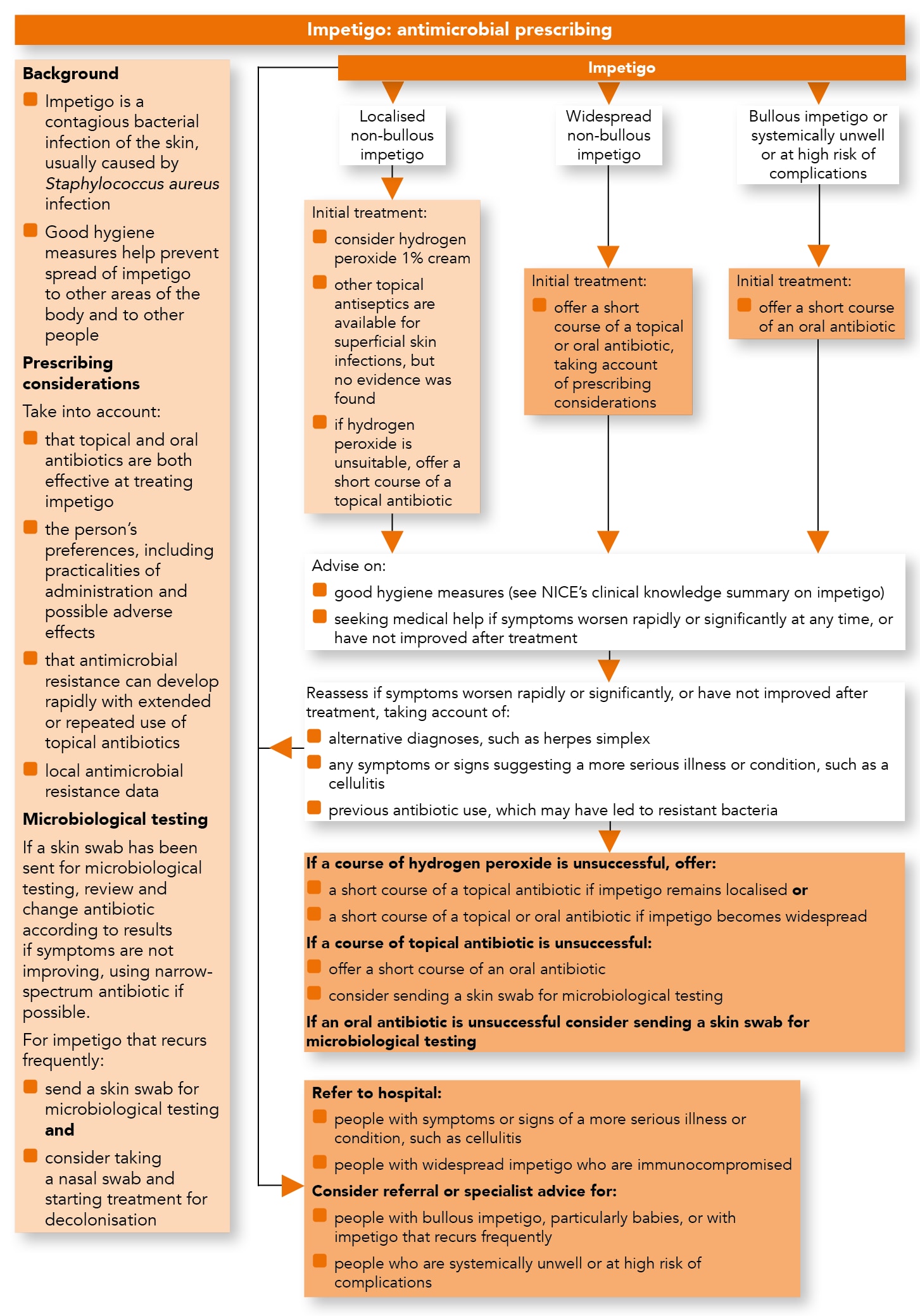
Algorithm 1: Impetigo—Antimicrobial Prescribing
Advice to Reduce the Spread of Impetigo
- Advise people with impetigo, and their parents or carers if appropriate, about good hygiene measures to reduce the spread of impetigo to other areas of the body and to other people.
Initial Treatment
Localised Non-bullous Impetigo
- Consider hydrogen peroxide 1% cream for people with localised non-bullous impetigo who are not systemically unwell or at high risk of complications (see recommendations on choice of antimicrobial). Although other topical antiseptics are available for treating superficial skin infections, no evidence was found for using them to treat impetigo
- If hydrogen peroxide 1% cream is unsuitable, offer a short course of a topical antibiotic for people with localised non-bullous impetigo who are not systemically unwell or at high risk of complications (see recommendations on choice of antimicrobial).
Widespread Non-bullous Impetigo
- Offer a short course of a topical or oral antibiotic for people with widespread non-bullous impetigo who are not systemically unwell or at high risk of complications (see recommendations on choice of antimicrobial). Take into account:
- that topical and oral antibiotics are both effective at treating impetigo
- the preferences of the person and, if appropriate, their parents or carers, including the practicalities of administration (particularly to large areas) and possible adverse effects
- previous use of topical antibiotics, because antimicrobial resistance can develop rapidly with extended or repeated use.
Bullous Impetigo or Impetigo in People Who Are Systemically Unwell or at High Risk of Complications
- Offer a short course of an oral antibiotic for:
- all people with bullous impetigo
- people with non-bullous impetigo who are systemically unwell or at high risk of complications.
Combination Treatment
- Do not offer combination treatment with a topical and oral antibiotic to treat impetigo.
Advice on Treatment
- Advise people with impetigo, and their parents or carers if appropriate, to seek medical help if symptoms worsen rapidly or significantly at any time, or have not improved after completing a course of treatment.
Reassessment and Further Treatment
- Reassess people with impetigo if their symptoms worsen rapidly or significantly at any time or have not improved after completing a course of treatment
- When reassessing people with impetigo, take account of:
- other possible diagnoses, such as herpes simplex
- any symptoms or signs suggesting a more serious illness or condition, such as cellulitis
- previous antibiotic use, which may have led to resistant bacteria
- For people with impetigo that is worsening or has not improved after treatment with hydrogen peroxide 1% cream, offer:
- a short course of a topical antibiotic if the impetigo remains localised or
- a short course of a topical or oral antibiotic if the impetigo has become widespread (see the recommendation on widespread non-bullous impetigo)
- For people with impetigo that is worsening or has not improved after completing a course of topical antibiotics:
- offer a short course of an oral antibiotic (see the recommendations on choice of antimicrobial) and
- consider sending a skin swab for microbiological testing
- For people with impetigo that is worsening or has not improved after completing a course of oral antibiotics, consider sending a skin swab for microbiological testing
- For people with impetigo that recurs frequently:
- send a skin swab for microbiological testing and
- consider taking a nasal swab and starting treatment for decolonisation
- If a skin swab has been sent for microbiological testing:
- review the choice of antibiotic when results are available and
- change the antibiotic according to results if symptoms are not improving, using a narrow-spectrum antibiotic if possible.
Referral and Seeking Specialist Advice
- Refer to hospital:
- people with impetigo and any symptoms or signs suggesting a more serious illness or condition (for example, cellulitis)
- people with widespread impetigo who are immunocompromised
- Consider referral or seeking specialist advice for people with impetigo if they:
- have bullous impetigo, particularly in babies (aged 1 year and under)
- have impetigo that recurs frequently
- are systemically unwell
- are at high risk of complications.
Choice of Antimicrobial
- When prescribing an antimicrobial for impetigo, take account of local antimicrobial resistance data when available and follow:
- table 1 for adults aged 18 years and over
- table 2 for children and young people under 18 years.
Table 1: Antimicrobials for Adults Aged 18 Years and Over
| Antimicrobial[A] | Dosage and Course Length[B] |
|---|---|
| Topical antiseptic | |
| Hydrogen peroxide 1%[C] | Apply two or three times a day for 5 days[D] |
| First-choice topical antibiotic[E] if hydrogen peroxide unsuitable (for example, if impetigo is around eyes) or ineffective | |
| Fusidic acid 2% | Apply three times a day for 5 days[D] |
| Alternative topical antibiotic[E] if fusidic acid resistance suspected or confirmed | |
| Mupirocin 2% | Apply three times a day for 5 days[D] |
| First-choice oral antibiotic | |
| Flucloxacillin | 500 mg four times a day for 5 days[D] |
| Alternative oral antibiotics if penicillin allergy or flucloxacillin unsuitable | |
| Clarithromycin | 250 mg twice a day for five days[D],[F] |
| Erythromycin (in pregnancy) | 250 mg to 500 mg four times a day for 5 days[D] |
| If MRSA suspected or confirmed | |
| Consult local microbiologist | |
[A] See BNF for appropriate use and dosing in specific populations, for example, hepatic impairment, renal impairment, pregnancy and breastfeeding. [B] Oral doses are for immediate-release medicines.[C] Other topical antiseptics are available for superficial skin infections, but no evidence was found for using these in impetigo. [D] A 5-day course is appropriate for most people with impetigo but can be increased to 7 days based on clinical judgement, depending on the severity and number of lesions. [E] As with all antibiotics, extended or recurrent use of topical fusidic acid or mupirocin may increase the risk of developing antimicrobial resistance. See BNF for more information. [F] Dosage can be increased to 500 mg twice a day, if needed for severe infections. | |
| Abbreviations: BNF=British National Formulary; MRSA=methicillin-resistant Staphylcoccus aureus. | |
Table 2: Antimicrobials for Children and Young People Aged Under 18 Years
| Antimicrobial[A] | Dosage and course length[B] |
|---|---|
| Topical antiseptic | |
| Hydrogen peroxide 1%[C] | Apply two or three times a day for 5 days[D] |
| First-choice topical antibiotic[E] if hydrogen peroxide unsuitable (for example, if impetigo is around eyes) or ineffective | |
| Fusidic acid 2% | Apply three times a day for 5 days[D] |
| Alternative topical antibiotic[E] if fusidic acid resistance suspected or confirmed | |
| Mupirocin 2%[F] | Apply three times a day for 5 days[D] |
| First-choice oral antibiotic | |
| Flucloxacillin (oral solution capsules[G]) | 1 month to 1 year: 62.5–125 mg four times a day for 5 days[D] 2–9 years: 125–250 mg four times a day for 5 days[D] 10–17 years: 250–500 mg four times a day for 5 days[D] |
| Alternative oral antibiotics if penicillin allergy or flucloxacillin unsuitable (for example, if oral solution unpalatable and unable to swallow capsules) | |
| Clarithromycin | 1 month to 11 years: Under 8 kg: 7.5 mg/kg twice a day for 5 days[D] 8–11 kg: 62.5 mg twice a day for 5 days[D] 12–19 kg: 125 mg twice a day for 5 days[D] 20–29 kg: 187.5 mg twice a day for 5 days[D] 30–40 kg: 250 mg twice a day for 5 days[D] 12–17 years: 250 mg twice a day for 5 days[D],[H] |
| Erythromycin (in pregnancy) | 8–17 years: 250–500 mg four times a day for 5 days[D] |
| If MRSA suspected or confirmed | |
| Consult local microbiologist | |
| [A] See BNF for Children for appropriate use and dosing in specific populations, for example, hepatic impairment, renal impairment, pregnancy and breastfeeding. Dosing in some age groups may be off-label. [B] Oral doses are for immediate-release medicines. The age bands apply to children of average size and, in practice, the prescriber will use the age bands in conjunction with other factors such as the severity of the condition being treated and the child’s size in relation to the average size of children of the same age. [C] Other topical antiseptics are available for superficial skin infections, but no evidence was found for using these in impetigo. [D] A 5-day course is appropriate for most people with impetigo but can be increased to 7 days based on clinical judgement, depending on the severity and number of lesions. [E] As with all antibiotics, extended or recurrent use of topical fusidic acid or mupirocin may increase the risk of developing antimicrobial resistance. See BNF for Children for more information. [F] Licenses for use in infants vary between products. See individual summaries of product characteristics for details. [G] See Medicines for Children, Helping your child to swallow tablets. [H] Dosage can be increased to 500 mg twice a day, if needed for severe infections. | |
| Abbreviations: BNF=British National Formulary; MRSA=methicillin-resistant Staphylococcus aureus. | |