

This guideline covers the diagnosis and management of diverticular disease in people aged 18 years and over. It does not include recommendations on:
- investigation of suspected acute diverticulitis in secondary care
- management of abcessess, bowel perforations, anastomosis and bowel resection for people with complicated acute diverticulitis (elective and emergency surgery)
- timing of surgery for complicated acute diverticulitis
- management of recurrent acute diverticulitis.
Diverticulosis
Management and Advice
- Tell people with diverticulosis that the condition is asymptomatic and no specific treatments are needed
- Advise people to eat a healthy, balanced diet including whole grains, fruit and vegetables. Tell them that:
- there is no need to avoid seeds, nuts, popcorn or fruit skins
- if they have constipation and a low-fibre diet, increasing their fibre intake gradually may minimise flatulence and bloating
- Advise people to drink adequate fluid if they are increasing their fibre intake, especially if there is a risk of dehydration
- Consider bulk-forming laxatives for people with constipation
- Tell people about the benefits of exercise, and weight loss if they are overweight or obese, and stopping smoking, in reducing the risk of developing acute diverticulitis and symptomatic disease.
Diverticular Disease
Symptoms and Signs
- Suspect diverticular disease if a person presents with one or both of the following:
- intermittent abdominal pain in the left lower quadrant with constipation, diarrhoea or occasional large rectal bleeds (the pain may be triggered by eating and relieved by the passage of stool or flatus)
- tenderness in the left lower quadrant on abdominal examinationBe aware that:
- in a minority of people and in people of Asian origin, pain and tenderness may be localised in the right lower quadrant
- symptoms may overlap with conditions such as irritable bowel syndrome, colitis and malignancy.
Investigations and Referral
- Do not routinely refer people with suspected diverticular disease unless:
- routine endoscopic and/or radiological investigations cannot be organised from primary care or
- colitis is suspected or
- the person meets the criteria for a suspected cancer pathway
- If the person meets the criteria for a suspected cancer pathway, refer by this route (see NICE’s guideline on suspected cancer: recognition and referral).
Management and Advice
- Do not offer antibiotics to people with diverticular disease
- Advise people to avoid non-steroidal anti-inflammatory drugs and opioid analgesia if possible, because they may increase the risk of diverticular perforation
- For advice on diet, fluid intake, stopping smoking, weight loss and exercise, follow the recommendations for diverticulosis, above
- Advise people that:
- the benefits of increasing dietary fibre may take several weeks to achieve
- if tolerated, a high-fibre diet should be maintained for life
- Consider bulk-forming laxatives if:
- a high-fibre diet is unacceptable to the person or it is not tolerated or
- the person has persistent constipation or diarrhoea
- Consider simple analgesia, for example paracetamol, as needed if the person has ongoing abdominal pain
- Consider an antispasmodic if the person has abdominal cramping
- If the person has persistent symptoms or symptoms that do not respond to treatment, think about alternative causes and investigate and manage appropriately.
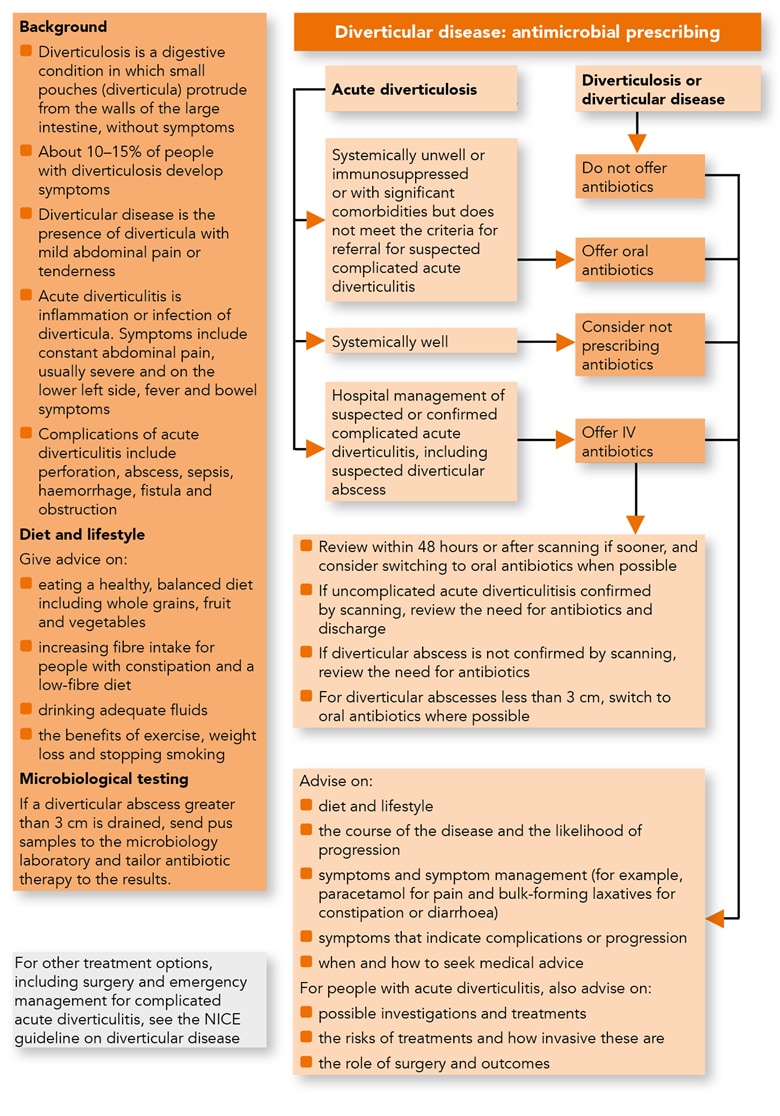
Algorithm 1: Diverticular Disease: Antimicrobial Prescribing
Acute Diverticulitis
Symptoms and Signs of Acute Diverticulitis
- Suspect acute diverticulitis if a person presents with constant abdominal pain, usually severe and localising in the left lower quadrant, with any of the following:
- fever or
- sudden change in bowel habit and significant rectal bleeding or passage of mucus from the rectum or
- tenderness in the left lower quadrant, a palpable abdominal mass or distention on abdominal examination, with a previous history of diverticulosis or diverticulitisBe aware that in a minority of people and in people of Asian origin, pain and tenderness may be localised in the right lower quadrant.
Symptoms and Signs of Complicated Acute Diverticulitis
- Suspect complicated acute diverticulitis and refer for same-day hospital assessment if the person has uncontrolled abdominal pain and any of the features in Table 1.
Table 1: Symptoms and Signs that Suggest Complicated Acute Diverticulitis
| Symptom or Sign | Possible Complication |
|---|---|
| Abdominal mass on examination or peri-rectal fullness on digital rectal examination | Intra-abdominal abscess |
| Abdominal rigidity and guarding on examination | Bowel perforation and peritonitis |
| Altered mental state, raised respiratory rate, low systolic blood pressure, raised heart rate, low tympanic temperature, no urine output or skin discolouration | Sepsis (see the NICE guideline on sepsis) |
| Faecaluria, pneumaturia, pyuria or the passage of faeces through the vagina | Fistula into the bladder or vagina |
| Colicky abdominal pain, absolute constipation (passage of no flatus or stool), vomiting or abdominal distention | Intestinal obstruction |
Investigation of Suspected Acute Diverticulitis
Primary Care
- For people with suspected uncomplicated acute diverticulitis who are not referred for same-day hospital assessment:
- reassess in primary care if their symptoms persist or worsen and
- consider referral to secondary care for further assessment.
For information on the non-surgical management of acute diverticulosis, see the diverticular disease antimicrobial prescribing algorithm in this summary.
- When prescribing an antibiotic for suspected or confirmed acute diverticulitis, follow the advice in Table 2.
Table 2: Antibiotics for Adults Aged 18 Years and Over With Suspected or Confirmed Acute Diverticulitis
| Antibiotic[1] | Dosage and Course Length[2] |
|---|---|
| First-choice oral antibiotic for suspected or confirmed uncomplicated acute diverticulitis | |
| Co‑amoxiclav | 500/125 mg three times a day for 5 days |
| Alternative first-choice oral antibiotics if penicillin allergy or co‑amoxiclav unsuitable | |
| Cefalexin (caution in penicillin allergy) with metronidazole | Cefalexin: 500 mg twice or three times a day (up to 1 to 1.5 g three or four times a day for severe infection) for 5 daysMetronidazole: 400 mg three times a day for 5 days |
| Trimethoprim with metronidazole | Trimethoprim: 200 mg twice a day for 5 days Metronidazole: 400 mg three times a day for 5 days |
| Ciprofloxacin (only if switching from IV ciprofloxacin with specialist advice; consider safety issues[3]) with metronidazole | Ciprofloxacin: 500 mg twice a day for 5 days Metronidazole: 400 mg three times a day for 5 days |
| First-choice intravenous antibiotics[4] for suspected or confirmed complicated acute diverticulitis | |
| Co‑amoxiclav | 1.2 g three times a day |
| Cefuroxime with metronidazole | Cefuroxime: 750 mg three or four times a day (increased to 1.5 g three or four times a day if severe infection) Metronidazole: 500 mg three times a day |
| Amoxicillin with gentamicin and metronidazole | Amoxicillin: 500 mg three times a day (increased to 1 g four times a day if severe infection) Gentamicin: Initially 5 to 7 mg/kg once a day, subsequent doses adjusted according to serum gentamicin concentration[5] Metronidazole: 500 mg three times a day |
| Ciprofloxacin[6] (consider safety issues[3]) with metronidazole | Ciprofloxacin: 400 mg twice or three times a day Metronidazole: 500 mg three times a day |
| Alternative intravenous antibiotics | |
| Consult local microbiologist | |
| [1] See BNF for appropriate use and dosing in specific populations, for example, hepatic impairment, renal impairment, pregnancy and breastfeeding, and administering intravenous (or, where appropriate, intramuscular) antibiotics. [2] A longer course may be needed based on clinical assessment. Continue antibiotics for up to 14 days in people with CT‑confirmed diverticular abscess. [3] See MHRA advice for restrictions and precautions for using fluoroquinolones due to very rare reports of disabling and potentially long-lasting or irreversible side effects affecting musculoskeletal and nervous systems. Warnings include: stopping treatment at first signs of a serious adverse reaction (such as tendonitis), prescribing with special caution for people over 60 years and avoiding coadministration with a corticosteroid (March 2019). [4] Review intravenous antibiotics within 48 hours or after scanning if sooner and consider stepping down to oral antibiotics where possible. [5] Therapeutic drug monitoring and assessment of renal function is required (BNF, August 2019). [6] Only in people with allergy to penicillins and cephalosporins. | |
Emergency Management of Complicated Acute Diverticulitis
- When prescribing an antibiotic for suspected or confirmed complicated acute diverticulitis, follow the advice in Table 2.
For information on the management of abcesses, see the full guideline.
Management of Recurrent Acute Diverticulitis
- Do not offer an aminosalicylate or antibiotics to prevent recurrent acute diverticulitis.