

Latest Guidance Updates21 November 2023: updated section on Postural Hypotension. Two new tables added to summarise blood pressure targets in the section on Monitoring Treatment and Blood Pressure Targets, as well as an updated recommendation on checking for postural hypotension in the same section. March 2022:
|
Overview
This Guidelines summary covers identifying and treating primary hypertension (high blood pressure) in people aged 18 years and over, including people with type 2 diabetes. It aims to reduce the risk of cardiovascular problems such as myocardial infarctions and strokes by helping healthcare professionals to diagnose hypertension accurately and treat it effectively. NICE has also produced a guideline on hypertension in pregnancy.This summary only covers recommendations for primary care. Refer to the full guideline for the complete set of recommendations.
Reflecting on Your Learnings
Reflection is important for continuous learning and development, and a critical part of the revalidation process for UK healthcare professionals. Click here to access the Guidelines Reflection Record.
Measuring Blood Pressure
- Ensure that healthcare professionals taking blood pressure measurements have adequate initial training and periodic review of their performance.
- Because automated devices may not measure blood pressure accurately if there is pulse irregularity (for example, due to atrial fibrillation), palpate the radial or brachial pulse before measuring blood pressure. If pulse irregularity is present, measure blood pressure manually using direct auscultation over the brachial artery.
- Healthcare providers must ensure that devices for measuring blood pressure are properly validated, maintained and regularly recalibrated according to manufacturers’ instructions. See the British and Irish Hypertension Society’s website for a list of validated blood pressure monitoring devices.
- When measuring blood pressure in the clinic or in the home, standardise the environment and provide a relaxed, temperate setting, with the person quiet and seated, and their arm outstretched and supported. Use an appropriate cuff size for the person’s arm.
- In people with symptoms of postural hypotension (falls or postural dizziness):
- measure blood pressure with the person either supine or seated
- measure blood pressure again with the person standing for at least 1 minute before measurement.
- If the systolic blood pressure falls by 20 mmHg or more when the person is standing:
- review medication
- measure subsequent blood pressures with the person standing
- consider referral to specialist care if symptoms of postural hypotension persist.
Postural Hypotension
- In people with symptoms of postural hypotension, including falls or postural dizziness:
- measure blood pressure with the person lying on their back (or consider a seated position, if it is inconvenient to measure blood pressure with the person lying down)
- measure blood pressure again after the person has been standing for at least 1 minute.
- If the person's systolic blood pressure falls by 20 mmHg or more, or their diastolic blood pressure falls by 10 mmHg or more, after the person has been standing for at least 1 minute:
- consider likely causes, including reviewing their current medication
- manage appropriately (for example, for advice on preventing falls in older people, see NICE's guideline on falls in older people: assessing risk and prevention
- measure subsequent blood pressures with the person standing
- consider referral to specialist care if symptoms of postural hypotension persist despite addressing likely causes.
- If the blood pressure drop is less than the thresholds in the above recommendation despite suggestive symptoms and the baseline measurement was previously taken from a seated position, repeat the measurements this time starting with the person lying on their back.
- Consider referring the person for further specialist assessment if blood pressure measurements do not confirm postural hypotension despite suggestive symptoms.
Diagnosing Hypertension
- When considering a diagnosis of hypertension, measure blood pressure in both arms:
- If the difference in readings between arms is more than 15 mmHg, repeat the measurements.
- If the difference in readings between arms remains more than 15 mmHg on the second measurement, measure subsequent blood pressures in the arm with the higher reading.
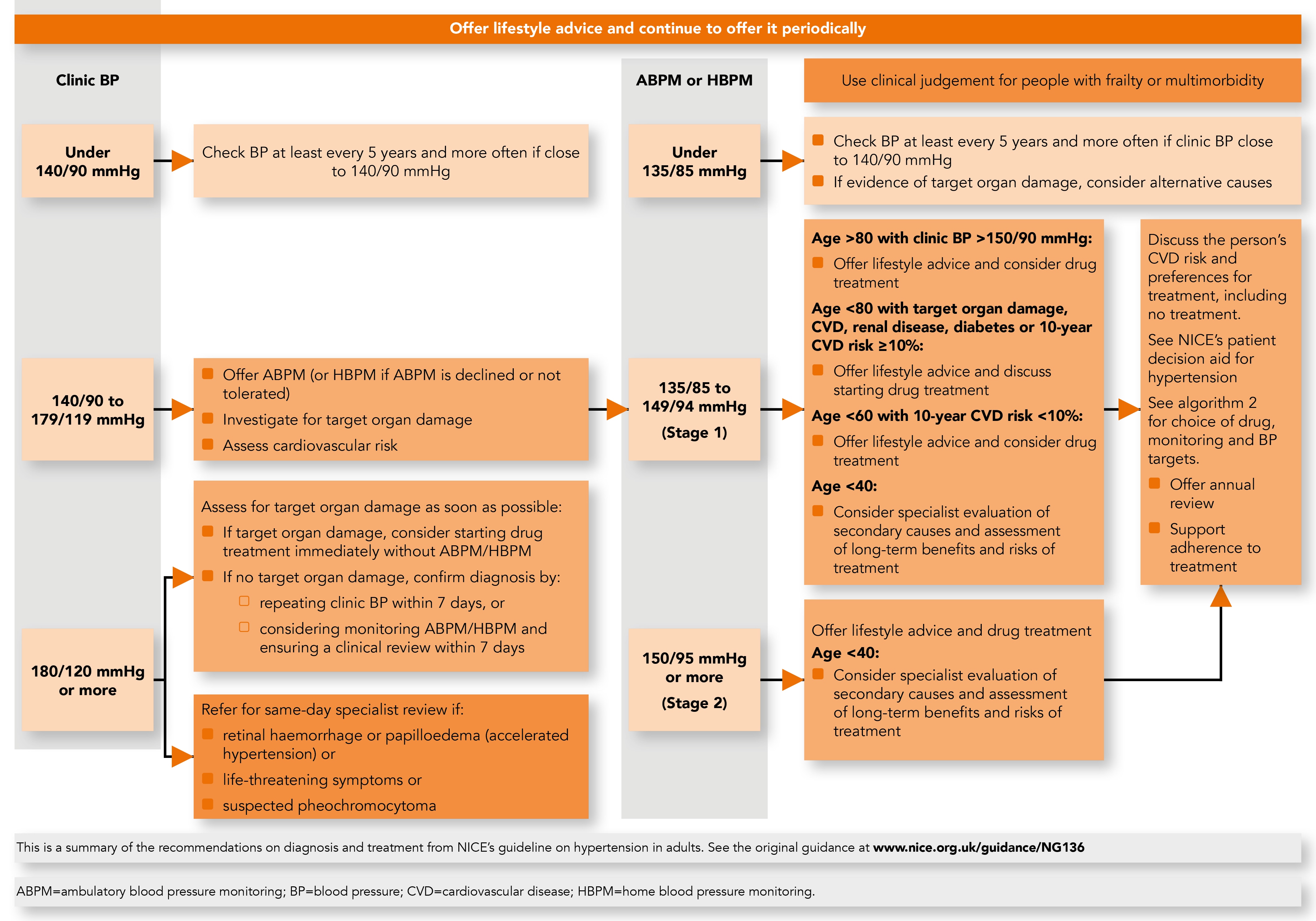
- If blood pressure measured in the clinic is 140/90 mmHg or higher:
- Take a second measurement during the consultation.
- If the second measurement is substantially different from the first, take a third measurement.
Record the lower of the last 2 measurements as the clinic blood pressure.
- If clinic blood pressure is between 140/90 mmHg and 180/120 mmHg, offer ambulatory blood pressure monitoring (ABPM) to confirm the diagnosis of hypertension. See the section on Identifying Who to Refer for Same-day Specialist Review of the full guideline for people with a clinic blood pressure 180/120 mmHg or higher.
- If ABPM is unsuitable or the person is unable to tolerate it, offer home blood pressure monitoring (HBPM) to confirm the diagnosis of hypertension.
- While waiting for confirmation of a diagnosis of hypertension, carry out:
- investigations for target organ damage (see the last recommendation in the section, Assessing Cardiovascular Risk and Target Organ Damage), followed by
- formal assessment of cardiovascular risk using a cardiovascular risk assessment tool (see the section on full formal risk assessment in NICE’s guideline on cardiovascular disease).
- When using ABPM to confirm a diagnosis of hypertension, ensure that at least 2 measurements per hour are taken during the person’s usual waking hours (for example, between 08:00 and 22:00). Use the average value of at least 14 measurements taken during the person’s usual waking hours to confirm a diagnosis of hypertension.
- When using HBPM to confirm a diagnosis of hypertension, ensure that:
- for each blood pressure recording, 2 consecutive measurements are taken, at least 1 minute apart and with the person seated and
- blood pressure is recorded twice daily, ideally in the morning and evening and
- blood pressure recording continues for at least 4 days, ideally for 7 days.
Discard the measurements taken on the first day and use the average value of all the remaining measurements to confirm a diagnosis of hypertension.
- Confirm diagnosis of hypertension in people with a:
- clinic blood pressure of 140/90 mmHg or higher and
- ABPM daytime average or HBPM average of 135/85 mmHg or higher.
- If hypertension is not diagnosed but there is evidence of target organ damage, consider carrying out investigations for alternative causes of the target organ damage (for information on investigations, see NICE’s guidelines on chronic kidney disease in adults and chronic heart failure).
- If hypertension is not diagnosed, measure the person’s clinic blood pressure at least every 5 years subsequently, and consider measuring it more frequently if the person’s clinic blood pressure is close to 140/90 mmHg.
Annual Blood Pressure Measurement for People With Type 2 Diabetes
- Measure blood pressure at least annually in an adult with type 2 diabetes without previously diagnosed hypertension or renal disease. Offer and reinforce preventive lifestyle advice.
Specialist Investigations for Possible Secondary Causes of Hypertension
- Consider the need for specialist investigations in people with signs and symptoms suggesting a secondary cause of hypertension.
Algorithm 1: Hypertension in Adults: Diagnosis and Management
Assessing Cardiovascular Risk and Target Organ Damage
For guidance on the early identification and management of chronic kidney disease, see NICE’s guideline on chronic kidney disease in adults.- Use a formal estimation of cardiovascular risk to discuss prognosis and healthcare options with people with hypertension, both for raised blood pressure and other modifiable risk factors.
- Estimate cardiovascular risk in line with the recommendations on identifying and assessing cardiovascular disease risk in NICE’s guideline on cardiovascular disease. Use clinic blood pressure measurements to calculate cardiovascular risk.
- For all people with hypertension offer to:
- test for the presence of protein in the urine by sending a urine sample for estimation of the albumin:creatinine ratio and test for haematuria using a reagent strip
- take a blood sample to measure glycated haemoglobin (HbA1C), electrolytes, creatinine, estimated glomerular filtration rate, total cholesterol and HDL cholesterol
- examine the fundi for the presence of hypertensive retinopathy
- arrange for a 12-lead electrocardiograph to be performed.
Treating and Monitoring Hypertension
Lifestyle Interventions
For guidance on the prevention of obesity and cardiovascular disease, see NICE’s guidelines on obesity prevention and cardiovascular disease prevention.
- Offer lifestyle advice to people with suspected or diagnosed hypertension, and continue to offer it periodically.
- Ask about people’s diet and exercise patterns because a healthy diet and regular exercise can reduce blood pressure. Offer appropriate guidance and written or audiovisual materials to promote lifestyle changes.
- Ask about people’s alcohol consumption and encourage a reduced intake if they drink excessively, because this can reduce blood pressure and has broader health benefits. See the recommendations for practice in NICE’s guideline on alcohol-use disorders.
- Discourage excessive consumption of coffee and other caffeine-rich products.
- Encourage people to keep their dietary sodium intake low, either by reducing or substituting sodium salt, as this can reduce blood pressure. Note that salt substitutes containing potassium chloride should not be used by older people, people with diabetes, pregnant women, people with kidney disease and people taking some antihypertensive drugs, such as ACE inhibitors and angiotensin II receptor blockers. Encourage salt reduction in these groups.
- Do not offer calcium, magnesium or potassium supplements as a method for reducing blood pressure.
- Offer advice and help smokers to stop smoking. See NICE’s guideline on tobacco.
- Inform people about local initiatives by, for example, healthcare teams or patient organisations that provide support and promote healthy lifestyle change, especially those that include group work for motivating lifestyle change.
Starting Antihypertensive Drug Treatment
NICE has produced a patient decision aid on treatment options for hypertension to help people and their healthcare professionals discuss the different types of treatment and make a decision that is right for each person.For advice on shared decision making for medicines, see the information on patient decision aids in NICE's guideline on medicines optimisation.
To support adherence and ensure that people with hypertension make the most effective use of their medicines, see NICE's guideline on medicines adherence.
- Offer antihypertensive drug treatment in addition to lifestyle advice to adults of any age with persistent stage 2 hypertension. Use clinical judgement for people of any age with frailty or multimorbidity (see also NICE’s guideline on multimorbidity).
- Discuss starting antihypertensive drug treatment, in addition to lifestyle advice, with adults aged under 80 with persistent stage 1 hypertension who have 1 or more of the following:
- target organ damage
- established cardiovascular disease
- renal disease
- diabetes
- an estimated 10-year risk of cardiovascular disease of 10% or more.
Use clinical judgement for people with frailty or multimorbidity (see also NICE’s guideline on multimorbidity).
- Discuss with the person their individual cardiovascular disease risk and their preferences for treatment, including no treatment, and explain the risks and benefits before starting antihypertensive drug treatment. Continue to offer lifestyle advice and support them to make lifestyle changes (see the section on Lifestyle Interventions), whether or not they choose to start antihypertensive drug treatment.
- Consider antihypertensive drug treatment in addition to lifestyle advice for adults aged under 60 with stage 1 hypertension and an estimated 10-year risk below 10%. Bear in mind that 10-year cardiovascular risk may underestimate the lifetime probability of developing cardiovascular disease.
- Consider antihypertensive drug treatment in addition to lifestyle advice for people aged over 80 with a clinic blood pressure of over 150/90 mmHg. Use clinical judgement for people with frailty or multimorbidity (see also NICE’s guideline on multimorbidity).
- For adults aged under 40 with hypertension, consider seeking specialist evaluation of secondary causes of hypertension and a more detailed assessment of the long-term balance of treatment benefit and risks.
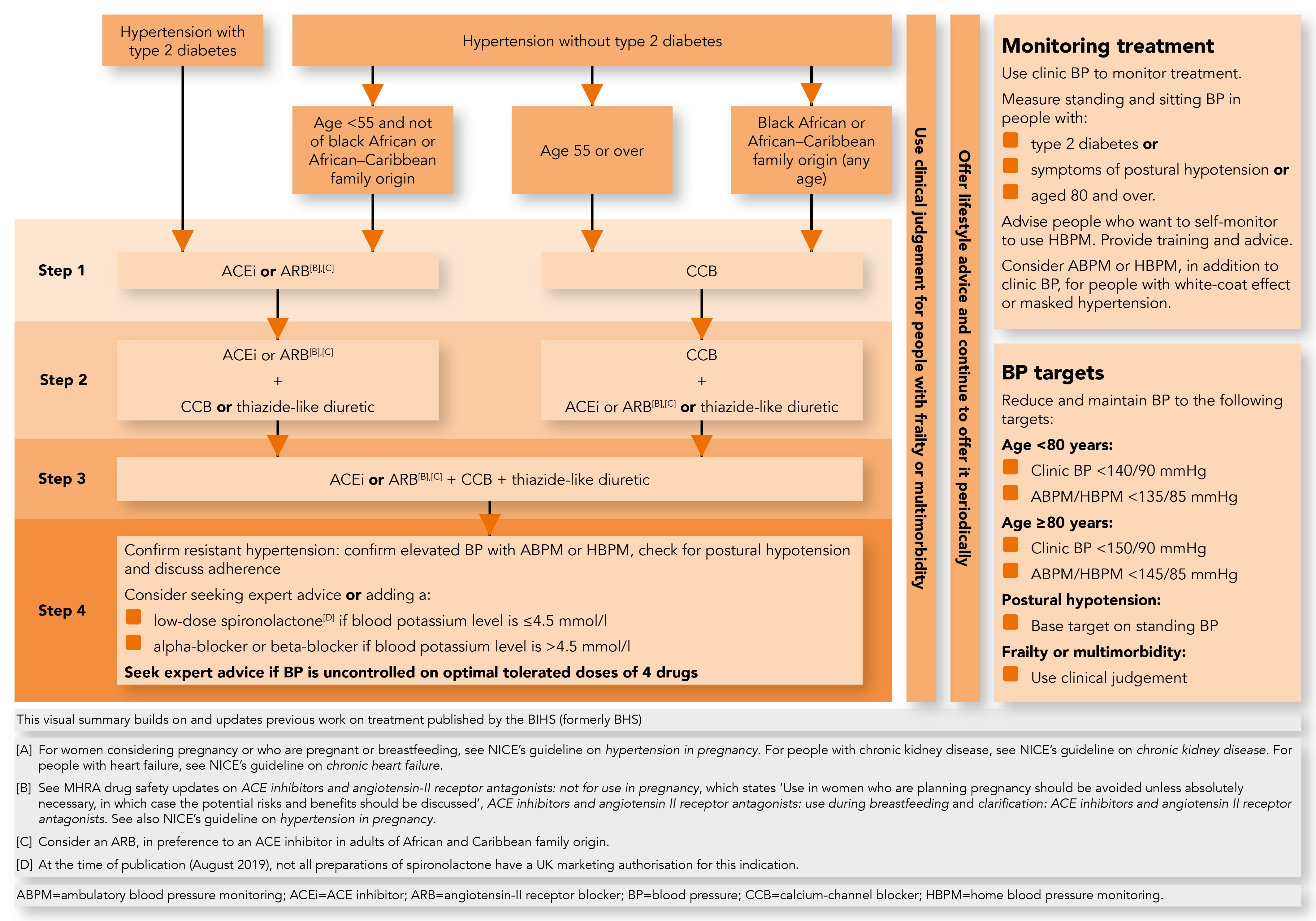
Algorithm 2: Choice of Antihypertensive Drug,[A] Monitoring Treatment and BP Targets
Monitoring Treatment and Blood Pressure Targets
For specific recommendations on blood pressure control in people with other conditions or who are pregnant, see NICE’s guidelines on chronic kidney disease, type 1 diabetes and hypertension in pregnancy.See also table 1 for clinic blood pressure targets for people aged under 80 and table 2 for clinic blood pressure targets for people aged 80 and over. The tables cover people with hypertension (with or without type 2 diabetes) as well as people with chronic kidney disease or type 1 diabetes.
Table 1: Clinic Blood Pressure Targets for People Aged Under 80
| Person under 80 with: | Clinic blood pressure target (systolic/diastolic mmHg) | Source |
| Below 140/90 | Recommendation 1.4.20 NICE's guideline on type 1 diabetes in adults (recommendation 1.13.8) NICE's guideline on chronic kidney disease (recommendation 1.6.1) |
| Below 130/80 | NICE's guideline on type 1 diabetes in adults (recommendation 1.13.8) NICE's guideline on chronic kidney disease (recommendation 1.6.2) |
Table 2: Clinic Blood Pressure Targets For People Aged 80 and Over
| Person aged 80 and over with: | Clinic blood pressure target (systolic/diastolic mmHg) | Source |
| Below 150/90 | Recommendation 1.4.21 NICE's guideline on type 1 diabetes in adults (recommendation 1.13.8) |
| Below 140/90 | NICE's guideline on chronic kidney disease (recommendation 1.6.1) |
| Below 130/80 | NICE's guideline on chronic kidney disease (recommendation 1.6.2) |
- Use clinic blood pressure measurements to monitor the response to lifestyle changes or drug treatment in people with hypertension.
- Check for postural hypotension (see the section on Postural Hypotension) in people with
hypertension and:- type 2 diabetes or
- symptoms of postural hypotension (see also recommendation 1.1.7) or
- aged 80 and over.
In people with a significant postural drop or symptoms of postural hypotension, treat to a blood pressure target based on standing blood pressure.
- Advise people with hypertension who choose to self-monitor their blood pressure to use HBPM (NHS England is supporting the use of HBPM through the blood pressure@home scheme).
- Consider ABPM or HBPM, in addition to clinic blood pressure measurements, for people with hypertension identified as having a white-coat effect or masked hypertension (in which clinic and non-clinic blood pressure results are conflicting). Be aware that the corresponding measurements for ABPM and HBPM are 5 mmHg lower than for clinic measurements (see the eighth recommendation in the section, Diagnosing Hypertension, for diagnostic thresholds).
- For people who choose to use HBPM, provide:
- training and advice on using home blood pressure monitors
- information about what to do if they are not achieving their target blood pressure.
Be aware that the corresponding measurements for HBPM are 5 mmHg lower than for clinic measurements (see the eighth recommendation in the section, Diagnosing Hypertension, for diagnostic thresholds).
- For adults with hypertension aged under 80, reduce clinic blood pressure to below 140/90 mmHg and ensure that it is maintained below that level. See also table 1 for guidance on clinic blood pressure targets for people aged under 80 with type 1 diabetes or severe chronic kidney disease.
- For adults with hypertension aged 80 and over, reduce clinic blood pressure to below 150/90 mmHg and ensure that it is maintained below that level. Use clinical judgement for people with frailty or multimorbidity (see also NICE’s guideline on multimorbidity). See also table 2 for guidance on clinic blood pressure targets for people aged 80 and over with type 1 diabetes or severe chronic kidney disease.
- When using ABPM or HBPM to monitor the response to treatment in adults with hypertension, use the average blood pressure level taken during the person’s usual waking hours (see the sixth and seventh recommendations in the section, Diagnosing Hypertension). Reduce blood pressure and ensure that it is maintained:
- below 135/85 mmHg for adults aged under 80
- below 145/85 mmHg for adults aged 80 and over.
Use clinical judgement for people with frailty or multimorbidity (see also NICE’s guideline on multimorbidity).
- Use the same blood pressure targets for people with and without cardiovascular disease.
- Provide an annual review of care for adults with hypertension to monitor blood pressure, provide people with support, and discuss their lifestyle, symptoms and medication.
Treatment Review When Type 2 Diabetes Is Diagnosed
- For an adult with type 2 diabetes on antihypertensive drug treatment when diabetes is diagnosed, review blood pressure control and medications used. Make changes only if there is poor control or if current drug treatment is not appropriate because of microvascular complications or metabolic problems.
Choosing Antihypertensive Drug Treatment (For People With or Without Type 2 Diabetes)
The recommendations in this section apply to people with hypertension with or without type 2 diabetes. They replace the recommendations on blood pressure management in NICE’s guideline on type 2 diabetes in adults. For guidance on choosing antihypertensive drug treatment in people with type 1 diabetes, see also the section on control of cardiovascular risk in NICE’s guideline on type 1 diabetes.Note that ACE inhibitors and angiotensin II receptor antagonists should not be used in pregnant or breastfeeding women or women planning pregnancy unless absolutely necessary, in which case the potential risks and benefits should be discussed. Follow the MHRA safety advice on ACE inhibitors and angiotensin II receptor antagonists: not for use in pregnancy, recommendations on how to use for breastfeeding and the related clarification on breastfeeding.
- For guidance on choice of hypertensive agent in people with chronic kidney disease, see NICE’s guideline on chronic kidney disease in adults. If possible, offer treatment with drugs taken only once a day.
- Prescribe non-proprietary drugs if these are appropriate and minimise cost.
- Offer people with isolated systolic hypertension (systolic blood pressure 160 mmHg or more) the same treatment as people with both raised systolic and diastolic blood pressure.
- Offer antihypertensive drug treatment to women of childbearing potential with diagnosed hypertension in line with the recommendations in this guideline. For women considering pregnancy or who are pregnant or breastfeeding, manage hypertension in line with the recommendations on management of pregnancy with chronic hypertension and breastfeeding in NICE’s guideline on hypertension in pregnancy.
- When choosing antihypertensive drug treatment for adults of black African or African–Caribbean family origin, consider an angiotensin II receptor blocker (ARB), in preference to an angiotensin-converting enzyme (ACE) inhibitor.
Follow the MHRA safety advice on ACE inhibitors and angiotensin II receptor antagonists: not for use in pregnancy, how to use for breastfeeding and clarification on breastfeeding. - For people with cardiovascular disease:
- Follow the recommendations for disease-specific indications in the NICE guideline on their condition (for example, when prescribing an ACE inhibitor or an ARB for secondary prevention of myocardial infarction). Relevant recommendations include:
- drug therapy for secondary prevention in the NICE guideline on acute coronary syndromes
- treatment after stabilisation in the NICE guideline on acute heart failure
- treating heart failure with reduced ejection fraction in the NICE guideline on chronic heart failure
- drugs for secondary prevention of cardiovascular disease in the NICE guideline on stable angina
- blood pressure management in the NICE guideline on type 1 diabetes in adults
- If their blood pressure remains uncontrolled, offer antihypertensive drug treatment in line with the recommendations in this section.
- Follow the recommendations for disease-specific indications in the NICE guideline on their condition (for example, when prescribing an ACE inhibitor or an ARB for secondary prevention of myocardial infarction). Relevant recommendations include:
Step 1 Treatment
- Offer an ACE inhibitor or an ARB to adults starting step 1 antihypertensive treatment who:
- have type 2 diabetes and are of any age or family origin (see also the fifth recommendation in the section, Choosing Antihypertensive Drug Treatment [For People With or Without Type 2 Diabetes] for adults of Black African or African–Caribbean family origin) or
- are aged under 55 but not of black African or African–Caribbean family origin.
Follow the MHRA safety advice on ACE inhibitors and angiotensin II receptor antagonists: not for use in pregnancy, how to use for breastfeeding and clarification on breastfeeding.
- If an ACE inhibitor is not tolerated, for example because of cough, offer an ARB to treat hypertension.
Follow the MHRA safety advice on ACE inhibitors and angiotensin II receptor antagonists: not for use in pregnancy, how to use for breastfeeding and clarification on breastfeeding. - Do not combine an ACE inhibitor with an ARB to treat hypertension.
- Offer a calcium-channel blocker (CCB) to adults starting step 1 antihypertensive treatment who:
- are aged 55 or over and do not have type 2 diabetes or
- are of Black African or African–Caribbean family origin and do not have type 2 diabetes (of any age).
- If a CCB is not tolerated, for example because of oedema, offer a thiazide-like diuretic to treat hypertension.
- If there is evidence of heart failure, offer a thiazide-like diuretic and follow NICE’s guideline on chronic heart failure.
- If starting or changing diuretic treatment for hypertension, offer a thiazide-like diuretic, such as indapamide in preference to a conventional thiazide diuretic such as bendroflumethiazide or hydrochlorothiazide.
- For adults with hypertension already having treatment with bendroflumethiazide or hydrochlorothiazide, who have stable, well-controlled blood pressure, continue with their current treatment.
Step 2 Treatment
- Before considering next step treatment for hypertension discuss with the person if they are taking their medicine as prescribed and support adherence in line with NICE’s guideline on medicines adherence.
- If hypertension is not controlled in adults taking step 1 treatment of an ACE inhibitor or ARB, offer the choice of 1 of the following drugs in addition to step 1 treatment:
- a CCB or
- a thiazide-like diuretic.
- If hypertension is not controlled in adults taking step 1 treatment of a CCB, offer the choice of 1 of the following drugs in addition to step 1 treatment:
- an ACE inhibitor or
- an ARB or
- a thiazide-like diuretic.
- If hypertension is not controlled in adults of Black African or African–Caribbean family origin who do not have type 2 diabetes taking step 1 treatment, consider an ARB, in preference to an ACE inhibitor, in addition to step 1 treatment.
Step 3 Treatment
- Before considering next step treatment for hypertension:
- review the person’s medications to ensure they are being taken at the optimal tolerated doses and
- discuss adherence (see the first recommendation under Step 2 Treatment).
- If hypertension is not controlled in adults taking step 2 treatment, offer a combination of:
- an ACE inhibitor or ARB (see also the first recommendation under Step 1 Treatment for people of Black African or African–Caribbean family origin) and
- a CCB and
- a thiazide-like diuretic.
Step 4 Treatment
- If hypertension is not controlled in adults taking the optimal tolerated doses of an ACE inhibitor or an ARB plus a CCB and a thiazide-like diuretic, regard them as having resistant hypertension.
- Before considering further treatment for a person with resistant hypertension:
- Confirm elevated clinic blood pressure measurements using ambulatory or home blood pressure recordings.
- Assess for postural hypotension.
- Discuss adherence (see the first recommendation under Step 2 Treatment).
- For people with confirmed resistant hypertension, consider adding a fourth antihypertensive drug as step 4 treatment or seeking specialist advice.
Follow the MHRA safety advice on ACE inhibitors and angiotensin II receptor antagonists: not for use in pregnancy, how to use for breastfeeding and clarification on breastfeeding. - Consider further diuretic therapy with low-dose spironolactone for adults with resistant hypertension starting step 4 treatment who have a blood potassium level of 4.5 mmol/l or less. Use particular caution in people with a reduced estimated glomerular filtration rate because they have an increased risk of hyperkalaemia.
In March 2019, this was an off-label use of some preparations of spironolactone. See NICE’s information on prescribing medicines. - When using further diuretic therapy for step 4 treatment of resistant hypertension, monitor blood sodium and potassium and renal function within 1 month of starting treatment and repeat as needed thereafter.
- Consider an alpha-blocker or beta-blocker for adults with resistant hypertension starting step 4 treatment who have a blood potassium level of more than 4.5 mmol/l.
- If blood pressure remains uncontrolled in people with resistant hypertension taking the optimal tolerated doses of 4 drugs, seek specialist advice.
Identifying Who to Refer for Same-day Specialist Review
- If a person has severe hypertension (clinic blood pressure of 180/120 mmHg or higher), but no symptoms or signs indicating same-day referral (see the second recommendation in this section), carry out investigations for target organ damage (see the last recommendation in the section, Assessing Cardiovascular Risk and Target Organ Damage) as soon as possible:
- If target organ damage is identified, consider starting antihypertensive drug treatment immediately, without waiting for the results of ABPM or HBPM.
- If no target organ damage is identified, confirm diagnosis by:
- repeating clinic blood pressure measurement within 7 days, or
- considering monitoring using ABPM (or HBPM if ABPM is not suitable or not tolerated), following the sixth and seventh recommendations in the section, Diagnosing Hypertension, and ensuring a clinical review within 7 days.
- Refer people for specialist assessment, carried out on the same day, if they have a clinic blood pressure of 180/120 mmHg and higher with:
- signs of retinal haemorrhage or papilloedema (accelerated hypertension) or
- life-threatening symptoms such as new onset confusion, chest pain, signs of heart failure, or acute kidney injury.
- Refer people for specialist assessment, carried out on the same day, if they have suspected phaeochromocytoma (for example, labile or postural hypotension, headache, palpitations, pallor, abdominal pain or diaphoresis).